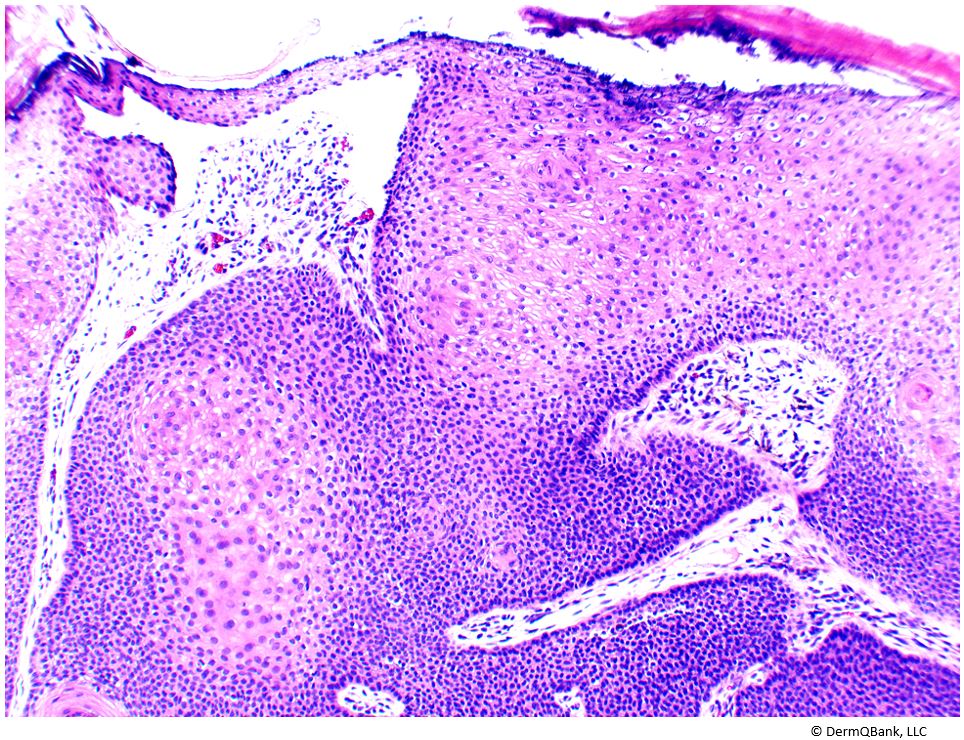
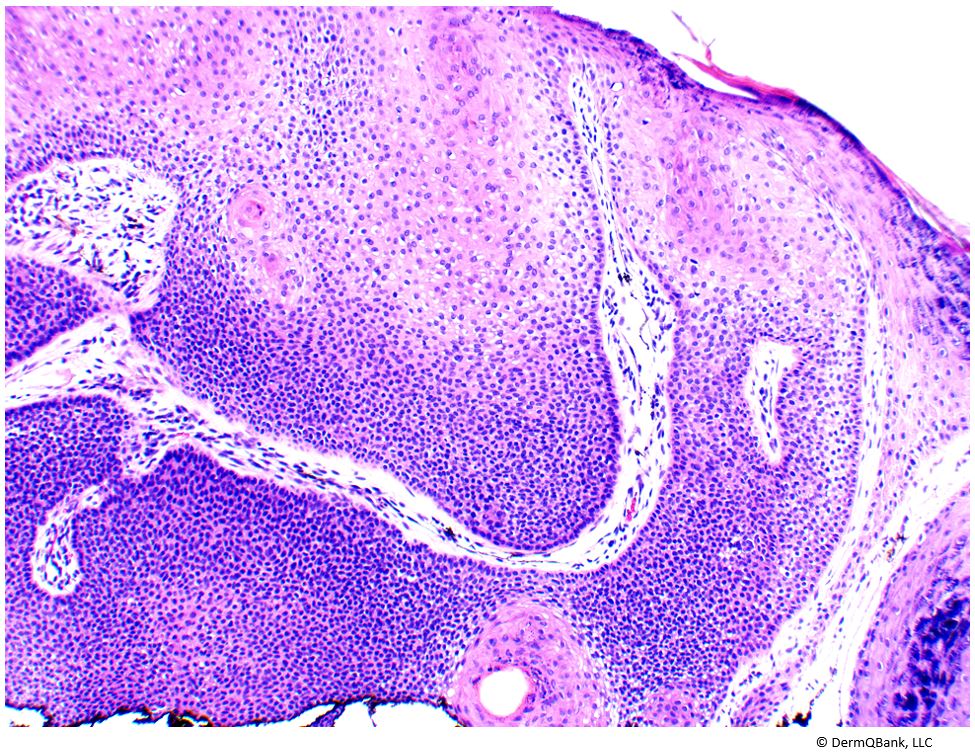
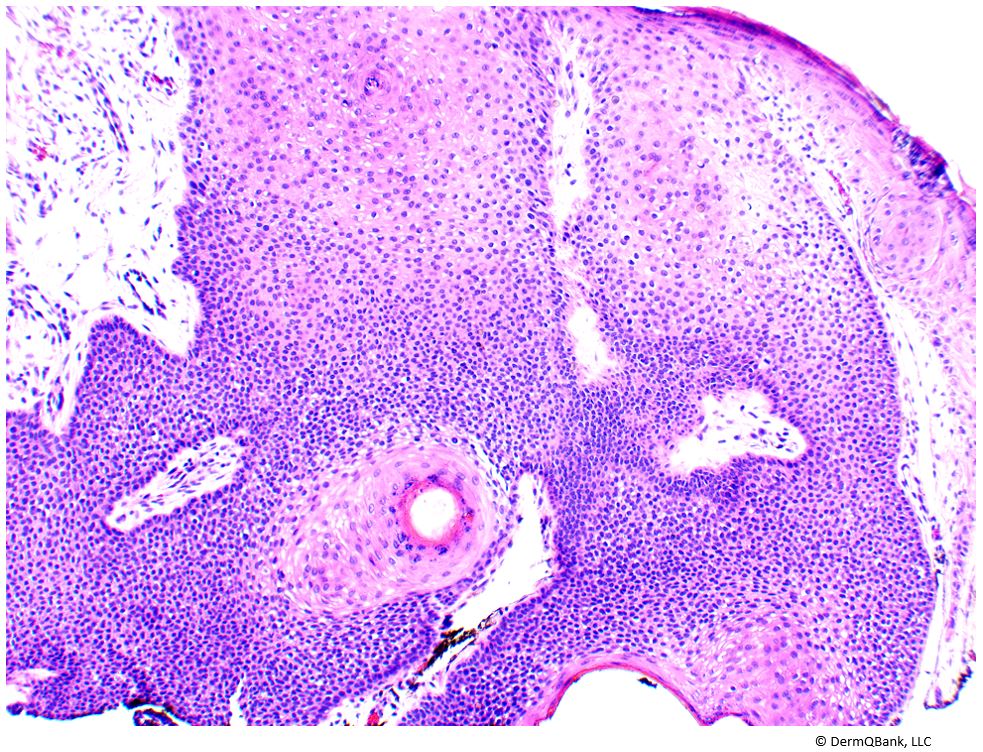
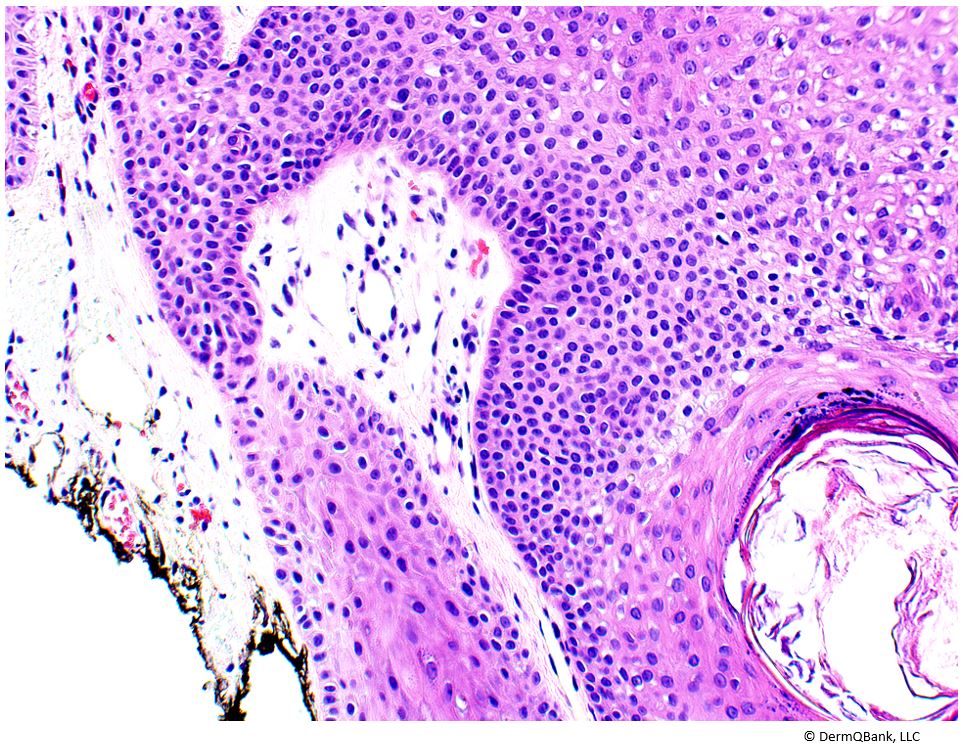
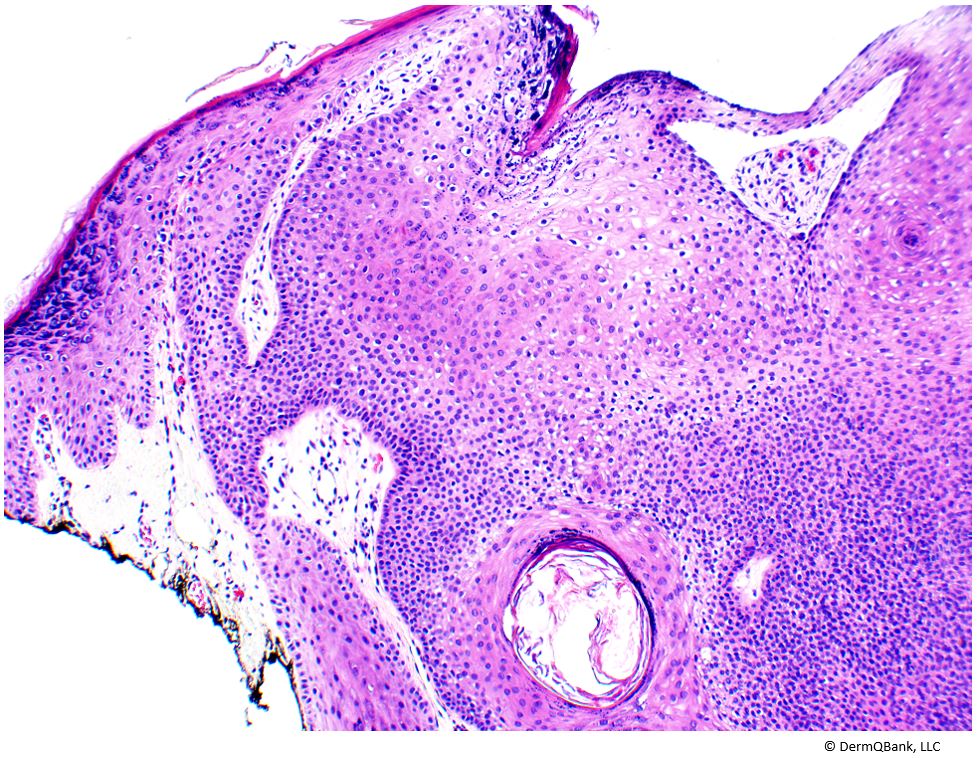
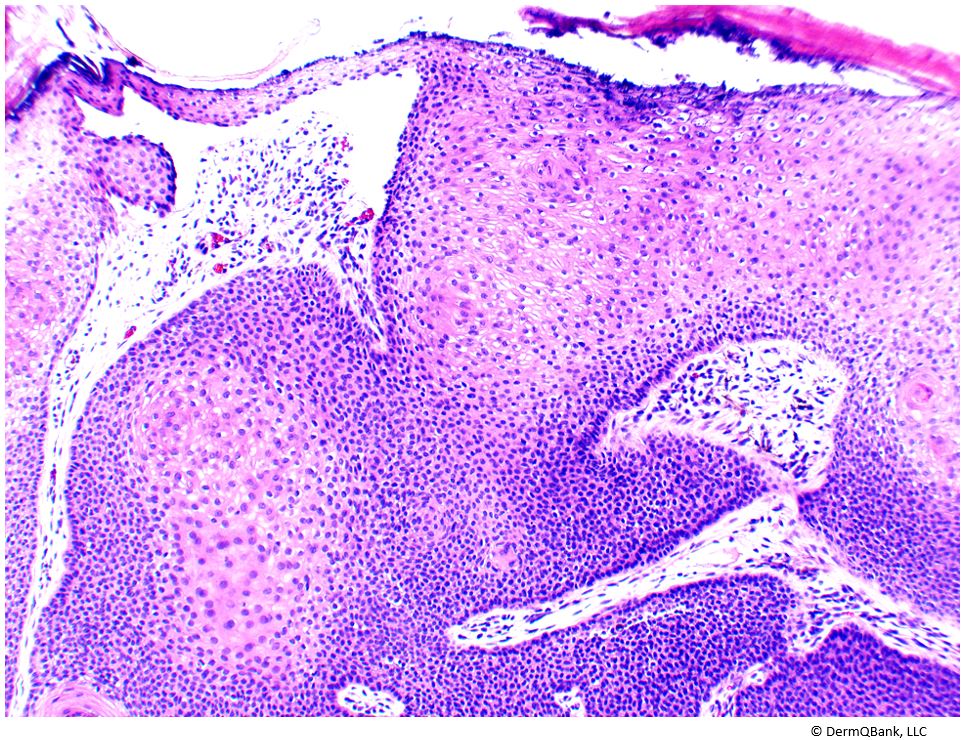
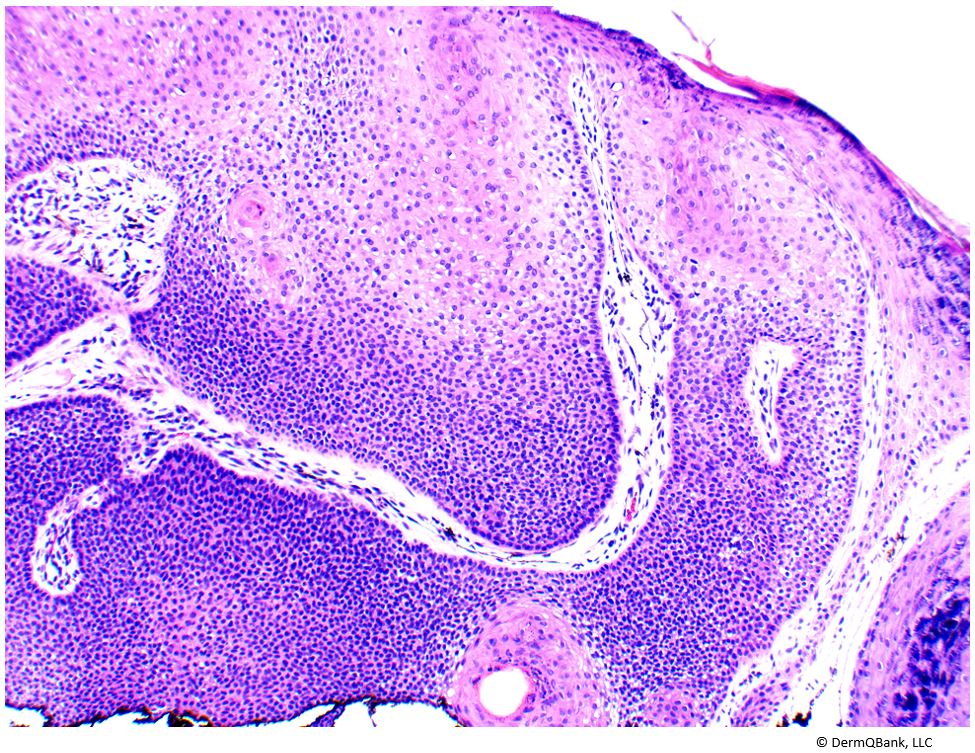
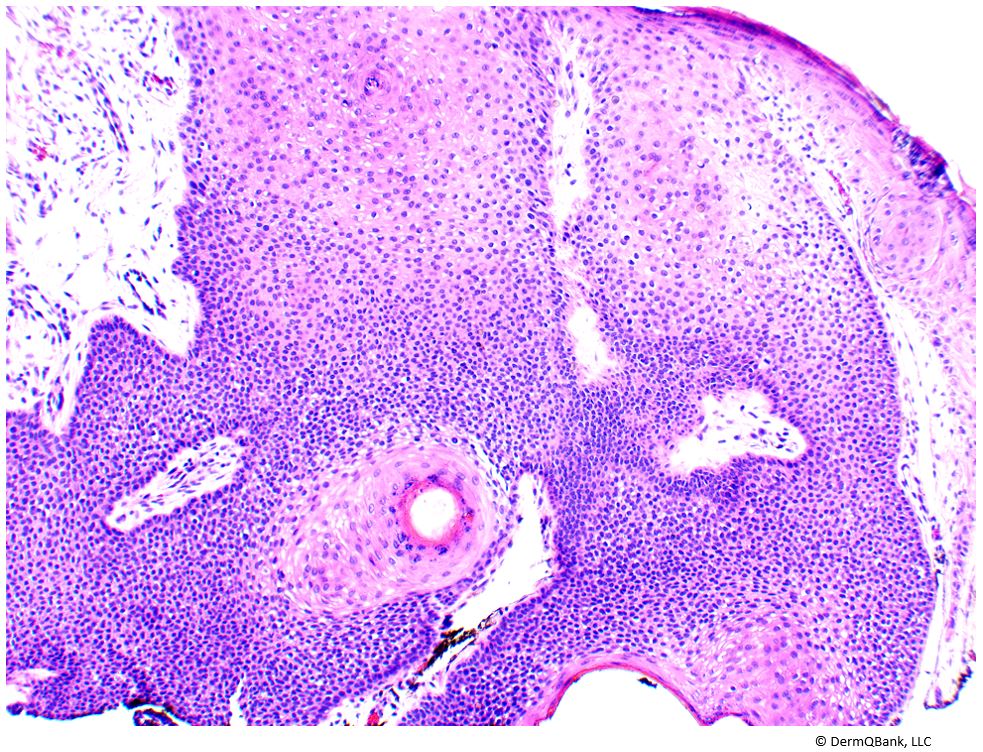
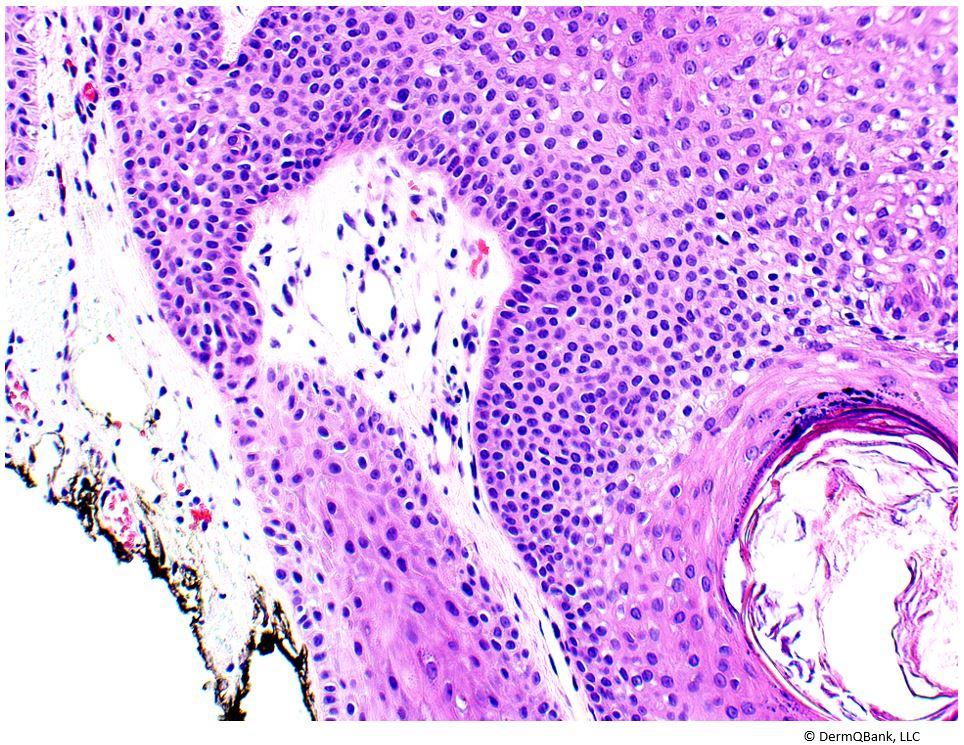
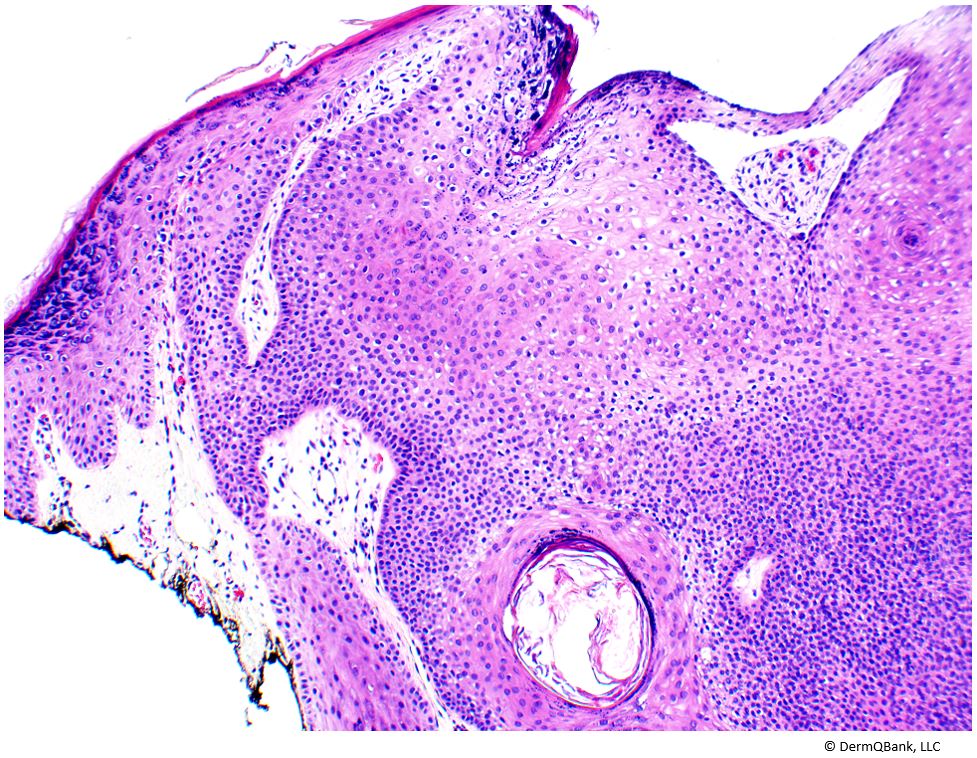
The pictured lesion is a trichilemmoma.
Cowden disease, or multiple hamartoma syndrome, is an autosomal dominant (AD) condition caused by a mutation in the tumor suppressor gene PTEN and is
characterized by multiple tumors of ectodermal, mesodermal, and endodermal
origin.
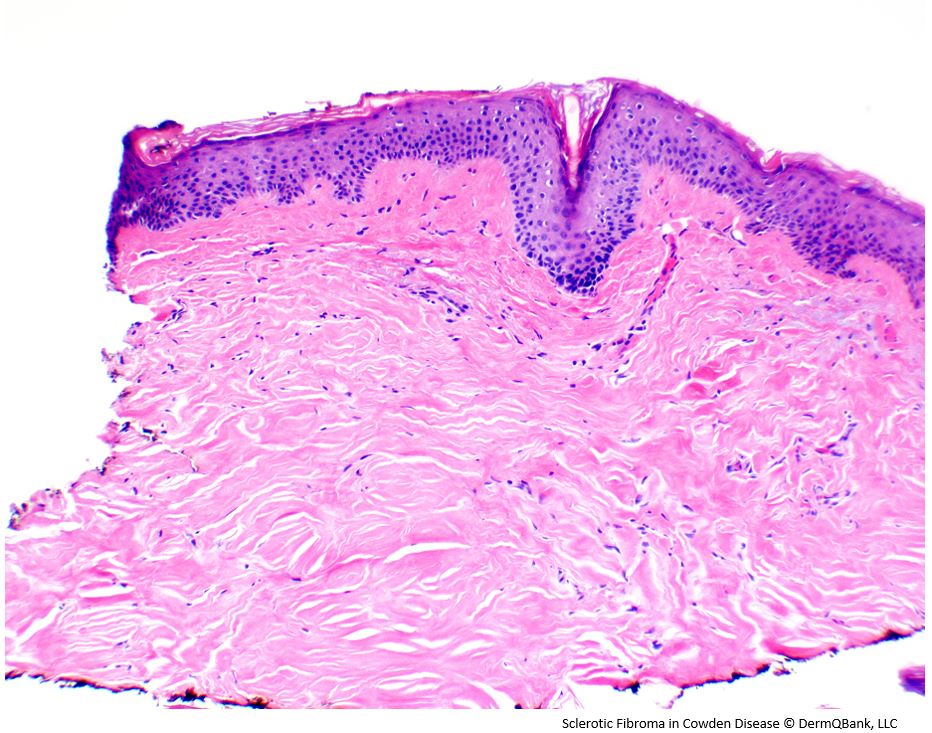
Major cutaneous features include facial trichilemmomas, oral
papillomas, acral keratotic papules, and sclerotic fibromas.
Major diagnostic criteria include biopsy proven trichilemmoma, multiple palmoplantar keratoses, multifocal or extensive oral mucosal papillomatosis, multiple cutaneous facial papules, pigmented macules on the glans penis, macrocephaly, breast carcinoma, thyroid carcinoma, endometrial carcinoma, and multiple gastrointestinal hamartomas or ganglioneuromas
(Pilarski et al. J Natl Cancer Inst 2013).
Histologically there is a downward
growth of the epidermis, forming large lobules with glycogen containing
keratinocytes giving them a clear appearance. There is a thin rim of palisaded
basal cells at the periphery of the downward growing epidermal nodule(s), which
sometimes exhibits a thickened basement membrane.
Clinical Pearl: Cowden disease is one of the PTEN hamartoma tumor syndromes. Common mucocutaenous manifestations include: trichilemmomas, multiple palmoplantar keratoses, multifocal or extensive oral mucosal papillomatosis, multiple cutaneous facial papules, and pigmented macules on the glans.